You've had this conversation before.
You're at work with a splitting headache. Your colleague pops two ibuprofen and is fine within an hour. You take the same tablet, wait, take another — and two hours later you're still squinting at your screen in pain. Or the opposite: your friend takes one tablet and feels drowsy for the rest of the day, while you feel absolutely nothing.
Same drug. Same dose. Completely different outcomes.
If you've spent years cycling through painkillers, trying different brands, doubling doses, or simply giving up and tolerating the pain — this isn't in your head, and it isn't bad luck. It's biology. Specifically, it's your genes.
The Part of Medicine No One Told You About
When a painkiller enters your body, it doesn't go straight to work. First, it has to be processed — absorbed, activated, and eventually cleared — by your liver. And this metabolic process is governed by a family of enzymes called Cytochrome P450 (CYP450).
Here's where it gets personal: tiny variations in your DNA, called Single Nucleotide Polymorphisms (SNPs), can make these enzymes work faster, slower, or not at all. And that single difference can completely change how a painkiller behaves in your body.
This field of science is called pharmacogenomics (PGx) — the study of how your genes determine your response to medication. It's been around for decades in research settings, but it's only now becoming accessible to everyday people in India.
Also Read: The Future of Personalized Medicine - The Role of Genetic Testing
Four Types of Metabolizers — Which One Are You?
Everyone falls into one of four categories, and your category determines everything about how a drug works for you:
| Metabolizer type | What happens in your body | What this feels like |
|---|---|---|
| Ultra-rapid | Your liver breaks down the drug so fast it's gone before it can work | The medication seems completely ineffective, no matter the dose |
| Normal (Extensive) | Your body processes the drug at a standard, expected rate | You experience the expected relief at a standard dose |
| Intermediate | Your liver works slower than average | The drug works, but side effects can creep in over time |
| Poor | Your liver processes the drug very slowly, causing it to accumulate | You feel intense side effects — nausea, drowsiness, or worse — from a standard dose |
Most people assume they're "normal." Many aren't. And in India, where genetic diversity across populations is remarkably high, the distribution of metaboliser types differs significantly from Western populations on which most drug dosage guidelines are based.
Let's Make This Concrete
Codeine is one of the most commonly prescribed painkillers in India, used for everything from dental procedures to post-surgical recovery. Here's what most people don't know: codeine is what's called a prodrug. It doesn't work in its original form. Your body has to convert it into morphine for it to relieve pain — and that conversion happens via an enzyme called CYP2D6.
If you're a poor metabolizer of CYP2D6, your body barely converts codeine to morphine. You get little to no pain relief, and your doctor may keep increasing your dose — with little benefit and growing frustration.
If you're an ultra-rapid metabolizer, the conversion happens too fast and too completely. The morphine floods your system. A standard dose becomes an overdose risk. There have been documented cases, including in children, of serious adverse reactions and even deaths from standard codeine doses in ultra-rapid metabolizers.
The same gene. The same drug. Life-changing differences.
Diclofenac, one of the most widely used NSAIDs in India, is processed through CYP2C9. Poor metabolizers of this enzyme accumulate the drug in their system, increasing the risk of gastric bleeding and kidney damage — even at prescribed doses.
Tramadol, naproxen, celecoxib — nearly every commonly used painkiller has a pharmacogenomic story like this.
Why This Matters More in India
Indian patients face a specific compounding problem. The vast majority of drug dosage guidelines were developed based on clinical trials conducted predominantly on Western, European populations. The genetic makeup of South Asian populations — particularly around CYP2C9, CYP2D6, and CYP3A5 — is meaningfully different.
This isn't a small variation. Studies have found that the frequency of certain "poor metabolizer" variants in the CYP2C9 gene is significantly higher in South Asian populations compared to Europeans. Prescribing European-derived standard doses to Indian patients, without any genetic context, is a gamble — often taken without the patient's knowledge.
If you live in India and have ever wondered why your response to a painkiller felt off, the answer may well be in your DNA.
What Does "Trial and Error" Actually Cost?
The traditional approach to finding the right painkiller is what doctors sometimes gently call empirical prescribing — which is a clinical way of saying "we try something and see what happens."
For pain management, this trial-and-error cycle carries real costs:
- Weeks or months of inadequate pain relief, affecting your sleep, productivity, and mental health
- Unnecessary side effects — nausea, gastric damage, drowsiness, or dependency — from drugs your body wasn't suited for
- Repeated doctor visits, investigation costs, and prescription changes
- Damage to organs from long-term use of drugs your body clears too slowly
- Distrust in medication — many people simply stop taking anything and learn to live with pain
None of this is inevitable.
Also Read: Why MedicaMap – Your Guide to Personalized Medicine
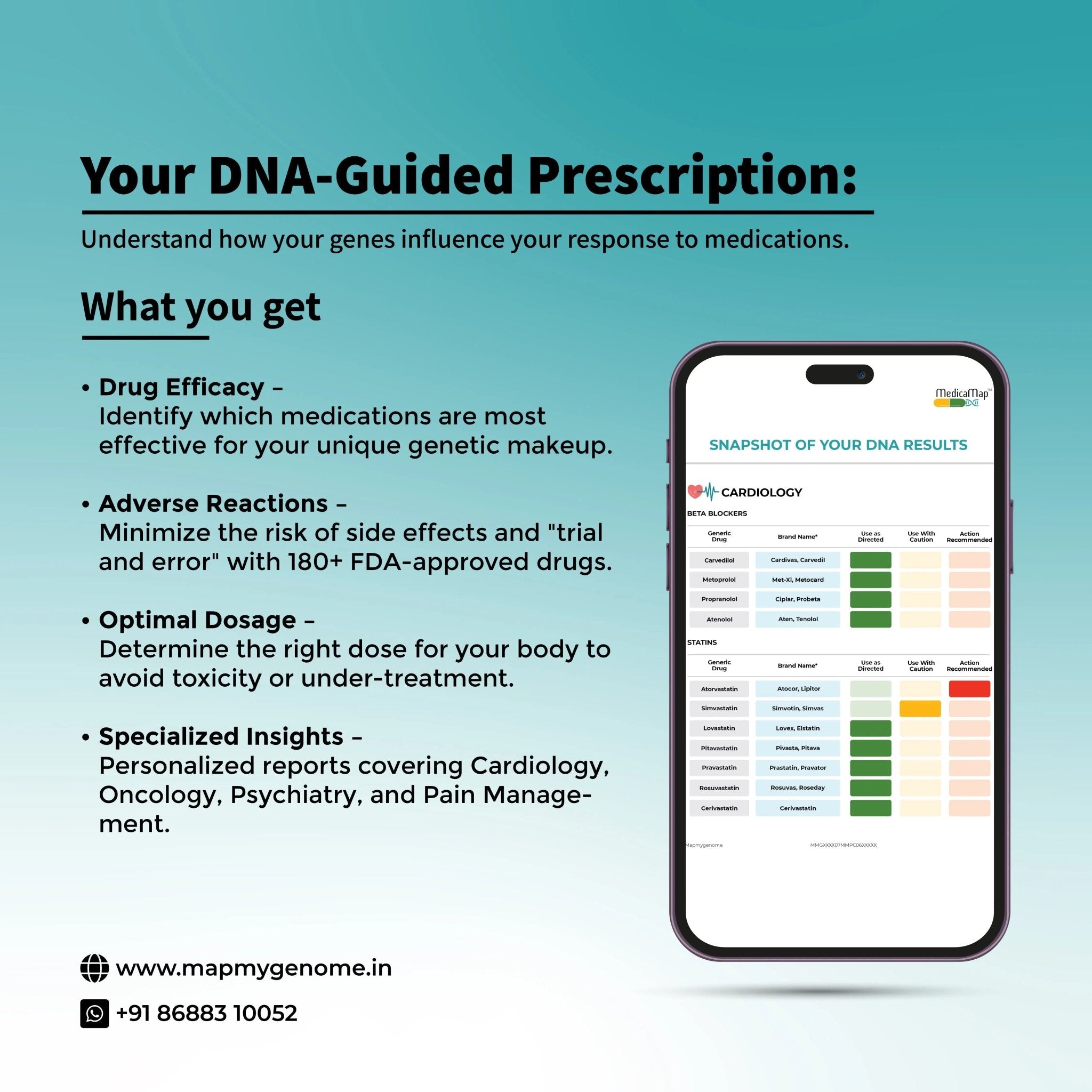
What Knowing Your Pharmacogenomic Profile Changes
A pharmacogenomic test analyses the specific genetic variants in your CYP450 enzymes and other drug-processing genes. The result isn't a diagnosis — it's a map. A permanent, one-time reference that tells your doctor how your body handles over 100 commonly prescribed drugs across multiple classes.
For pain management specifically, this map answers questions like:
- Is codeine likely to be effective for you, or should your doctor choose an alternative from the start?
- Are you at elevated risk of diclofenac-induced gastric damage?
- How should your dose of tramadol be adjusted for your metaboliser status?
- Which NSAIDs are likely to work fastest with the fewest side effects for your specific genetic profile?
Instead of your doctor choosing a painkiller based on general guidelines and hoping for the best, they can choose one that fits your biology from the first prescription.
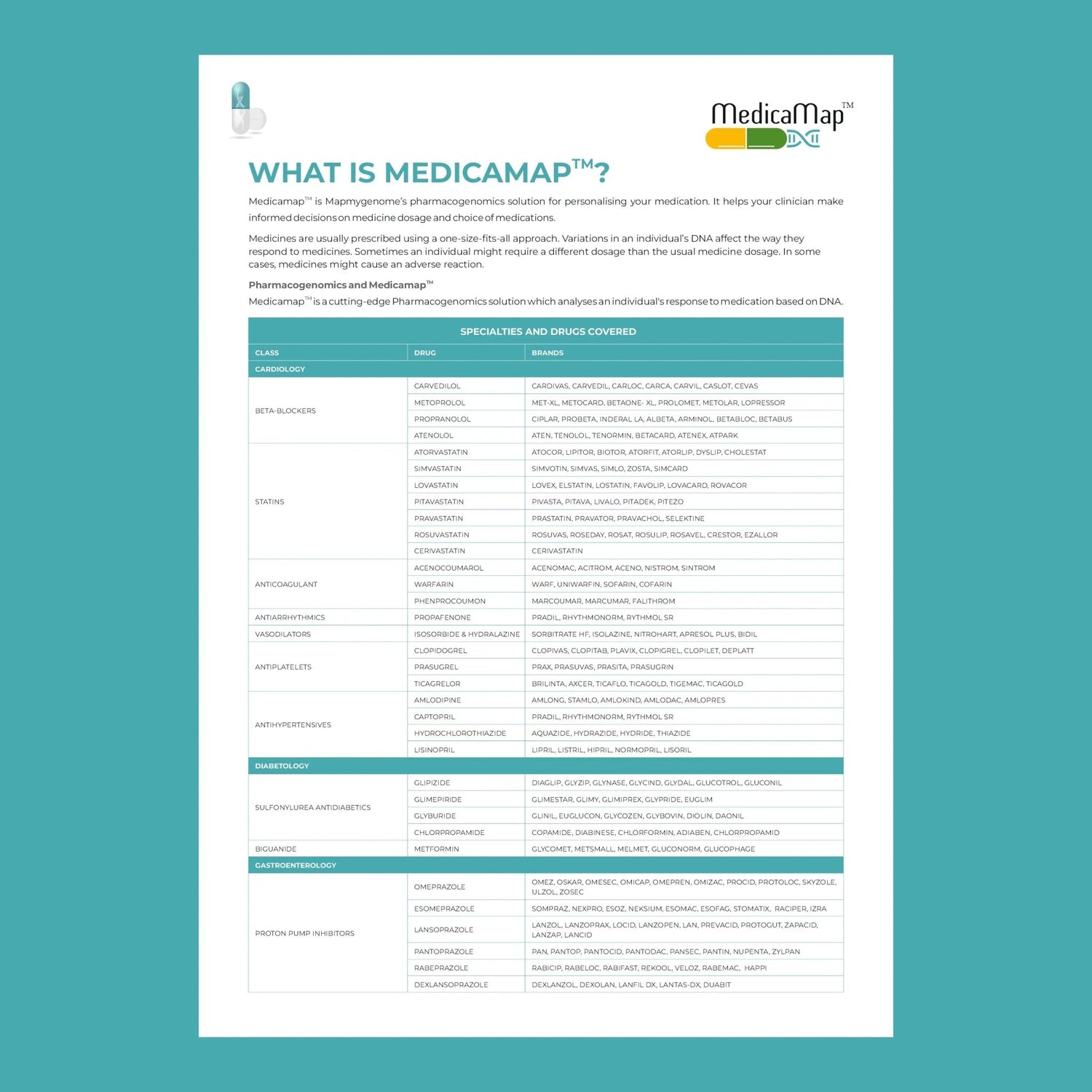
MedicaMap™: Your Genetic Drug Response Profile
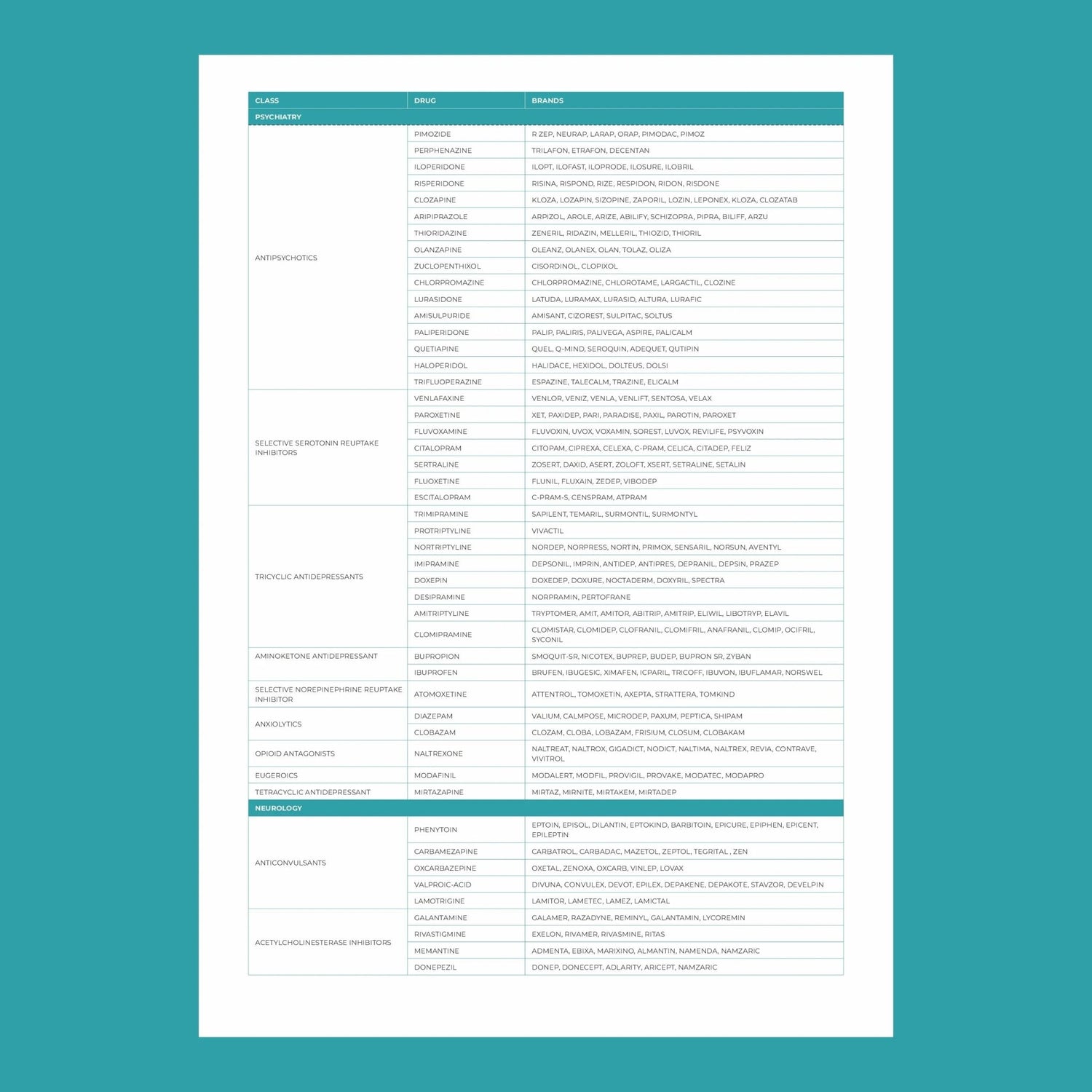
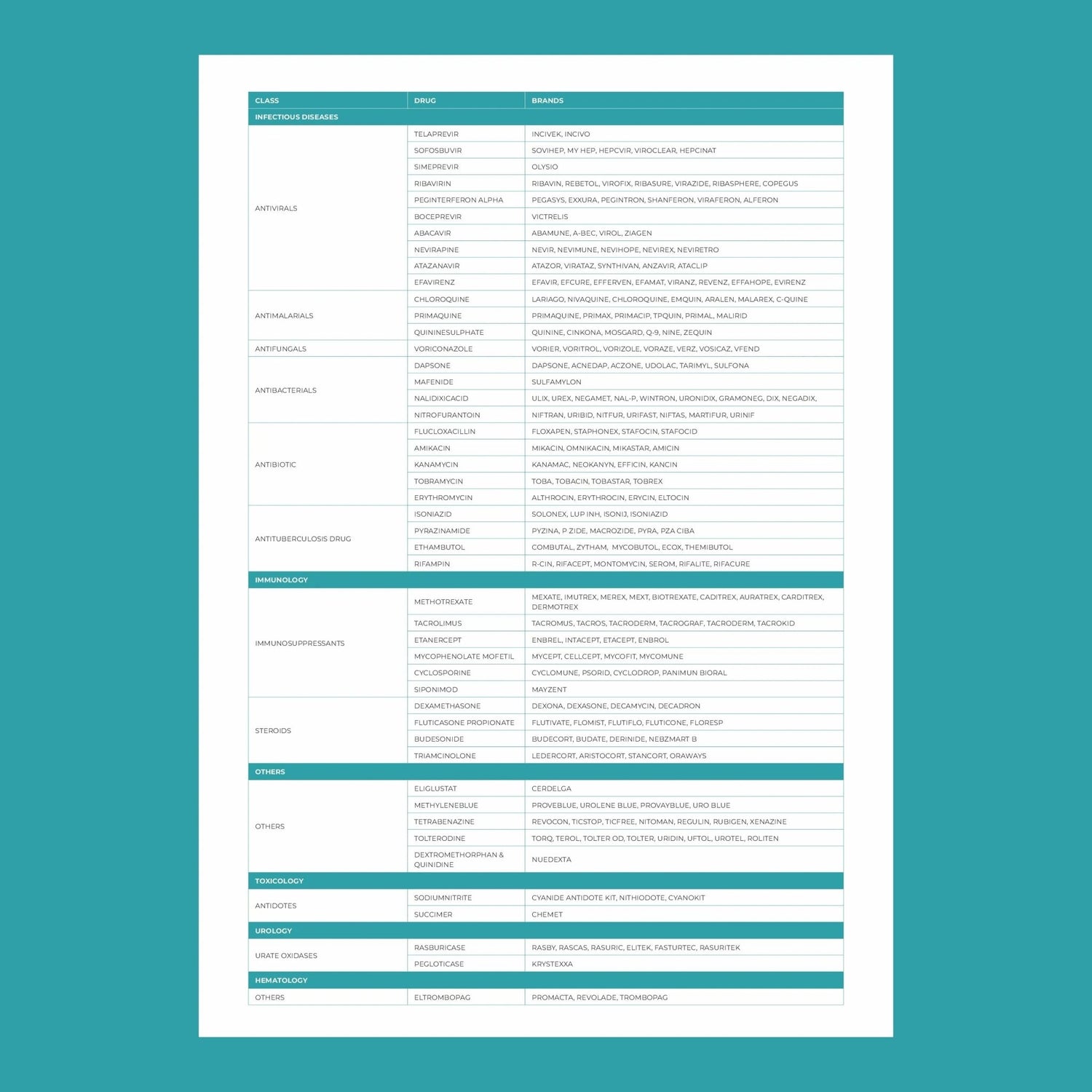
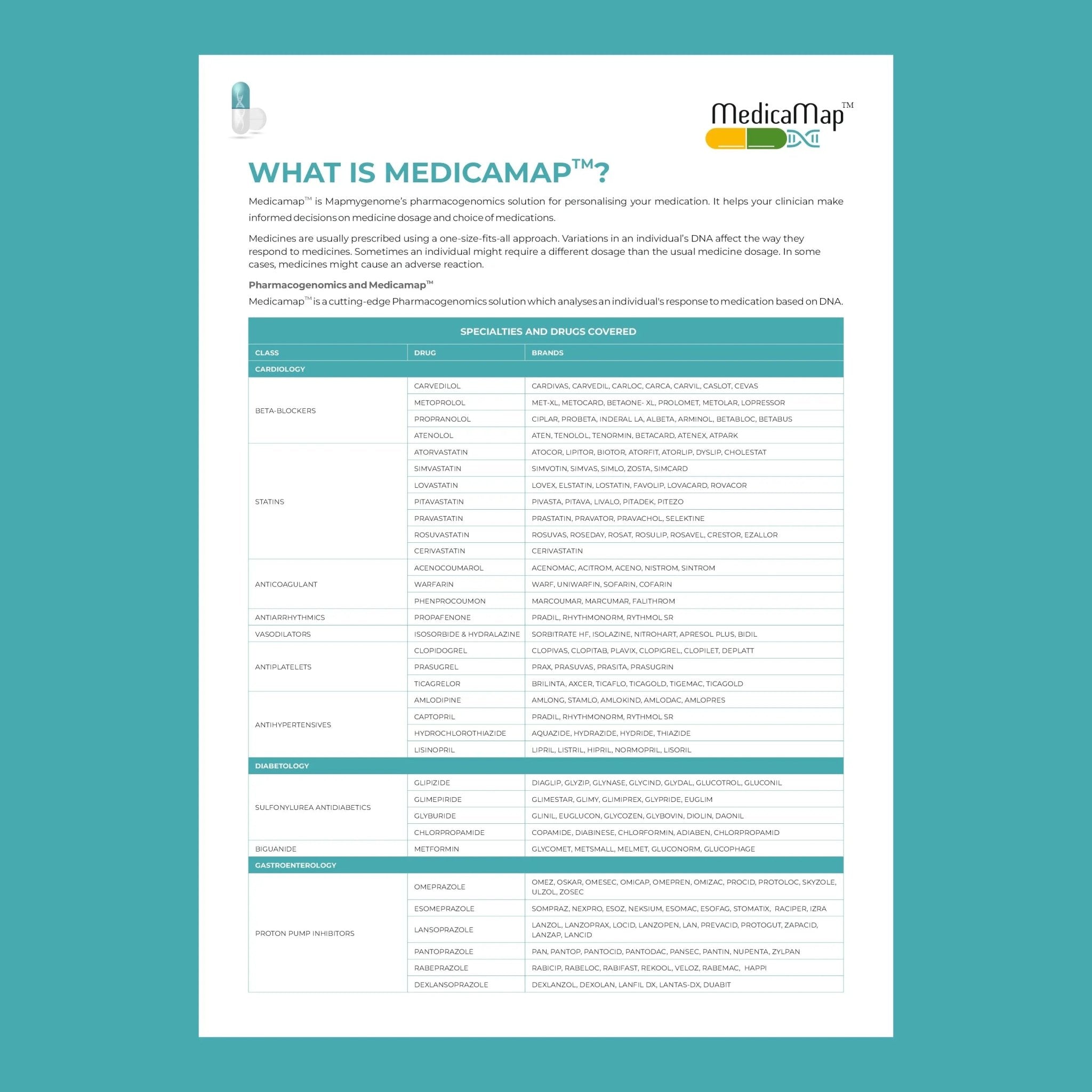
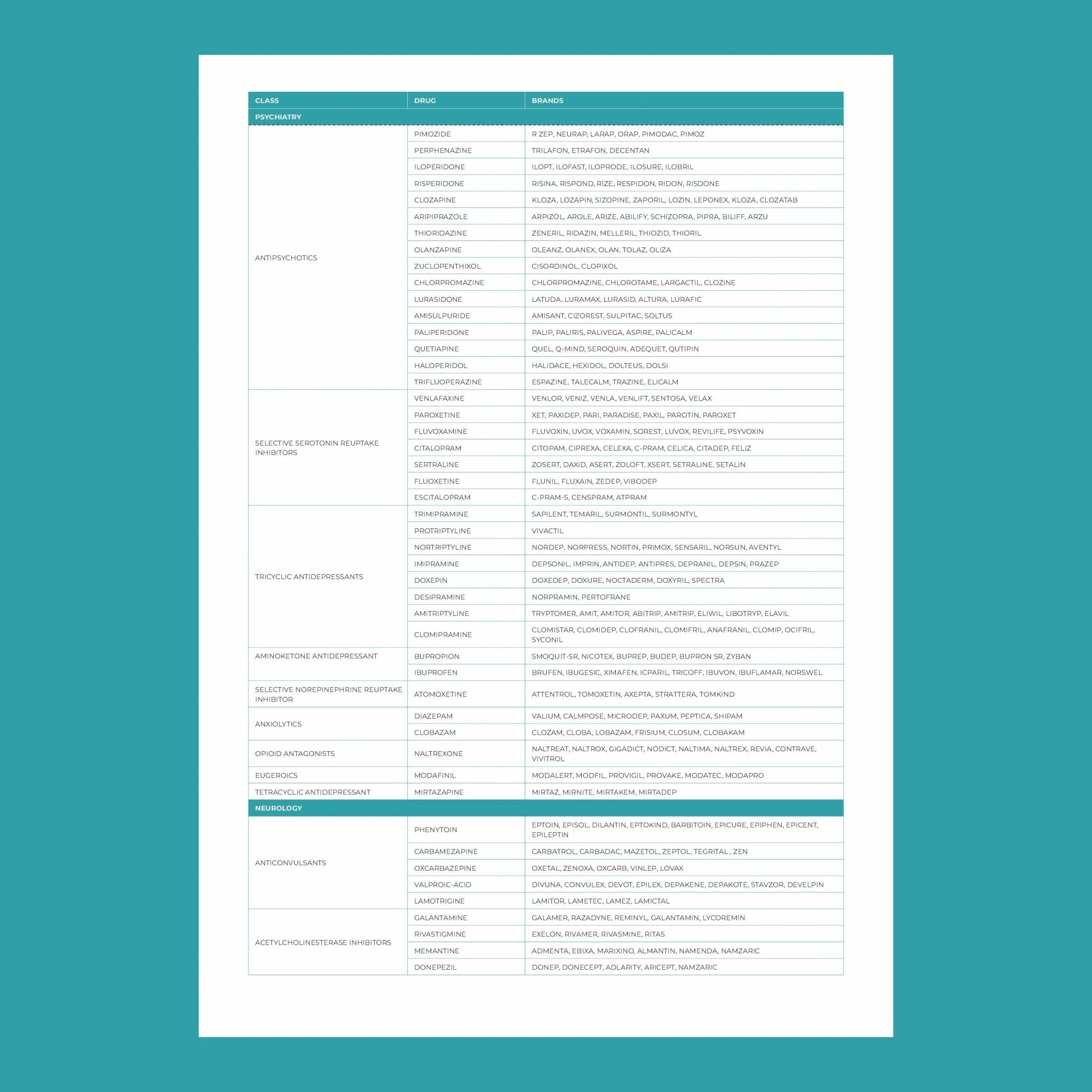
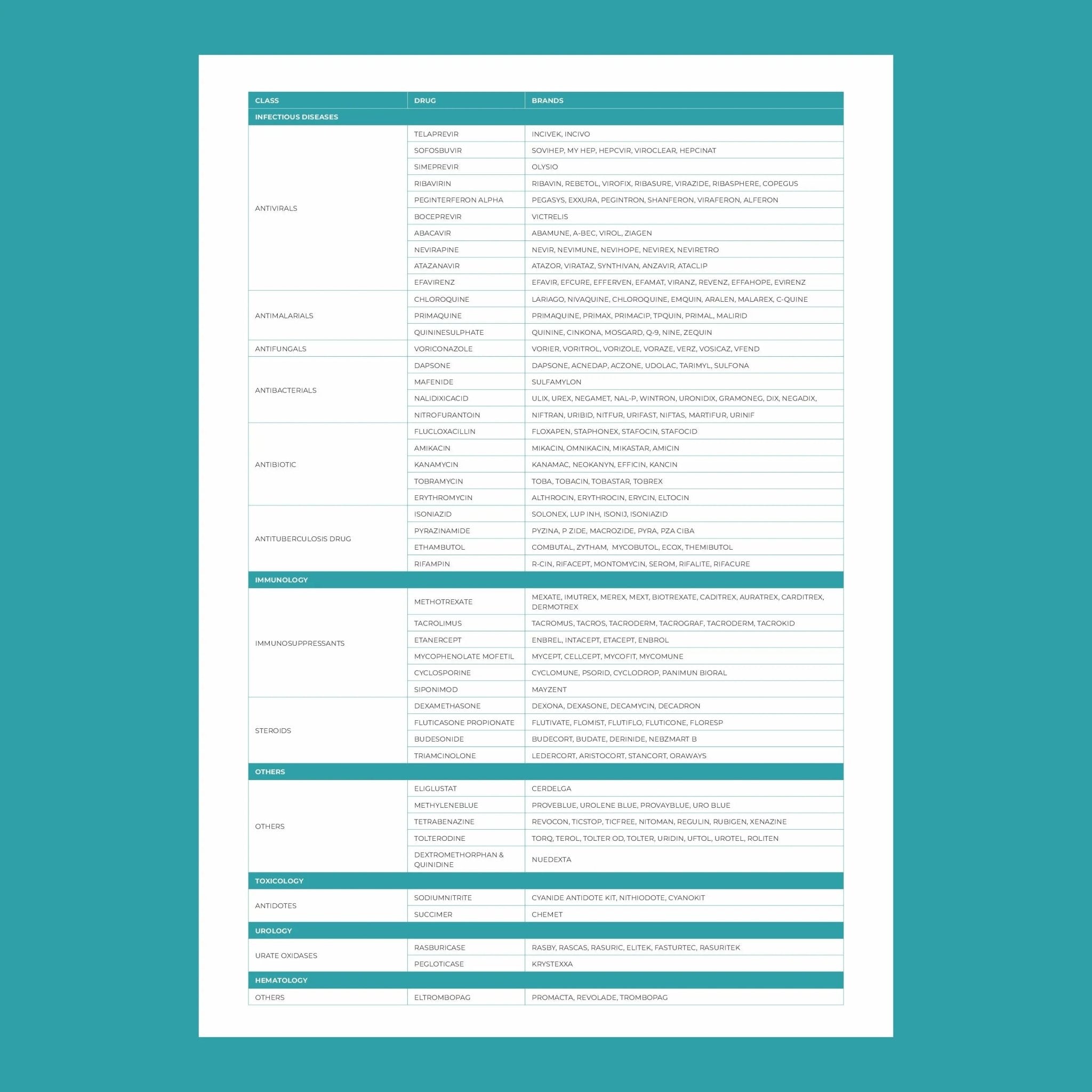
MapmyGenome's MedicaMap™ is designed exactly for this. Using a simple, non-invasive saliva sample collected at home, MedicaMap analyses your pharmacogenomic profile and generates a comprehensive report covering your body's response to 165+ US FDA-approved drugs across 12 specialties — including pain management, psychiatry, cardiology, and oncology.
The report is processed in NABL and CAP-accredited laboratories and structured using internationally recognised clinical guidelines, making it straightforward for your doctor or specialist to interpret and act on.
What MedicaMap™ gives you:
- Your metabolizer status for the key CYP450 enzymes that govern painkiller metabolism (CYP2C9, CYP2D6, CYP3A4/5, and others)
- Drug-specific guidance — which painkillers are likely to work, which to avoid, and where dosage adjustments may be needed
- A permanent medical reference you can share with any doctor, at any point in your life, for any future prescription
Because your genes don't change. Once you know, you always know.
Signs That Your Pharmacogenomic Profile May Be Working Against You
If several of these sound familiar, a pharmacogenomic test is worth serious consideration:
- Standard doses of painkillers consistently feel either too weak or too strong
- You've had unexplained adverse reactions to medications — nausea, dizziness, extreme drowsiness — at normal doses
- You need unusually high doses to feel any effect from a drug
- You've been through multiple painkiller prescriptions without finding one that works reliably
- A family member has had a serious or unexpected drug reaction
- You're managing a chronic pain condition and want a smarter, safer long-term approach
The Shift That's Coming
Pharmacogenomic testing is already standard of care for several drug classes in parts of Europe, North America, and Southeast Asia. Hospitals and cancer centres in India are beginning to adopt it for chemotherapy and cardiac medications. Pain management is the next frontier — and the tools to access it are available now, without waiting for your hospital to catch up.
You don't have to keep guessing. The reason a painkiller doesn't work for you isn't willpower, tolerance, or bad luck. It's written in your DNA — and now you can read it.
Ready to find out your metaboliser profile? Explore MedicaMap™ — MapmyGenome's at-home pharmacogenomic test, with a personalised report and a genetic counselling session included.
Know Your Body. Choose the Right Treatment.
Your genes determine how you respond to medication — and also your long-term disease risk. The Stay Young Bundle pairs Genomepatri DNA health screening with MapmyBiome gut testing, giving you a complete picture of your biology so every health decision is informed, not guesswork.